
As physical therapists, we are aware of the importance of adequate amounts of ankle dorsiflexion. It is essential for proper gait mechanics, negotiating stairs, performing squats and sit to stand transfers, jumping and landing, etc.
Evidence has shown that poor ankle mobility can increase risk of injury in athletes and non-athletes, leading to injuries to the Achillies (acute and chronic), ACL and patella tendon injuries.
How do you determine if your patient has enough ankle dorsiflexion? There are many ways to measure dorsiflexion, including open and closed-kinetic chain measurements.
One of my favorites is the Knee to Wall Lunge Test. I prefer this test since it is reliable and can be used to assist in determining likely dysfunctions and target initial treatment.
The Knee to Wall Lunge Test
For those who are not familiar with this test:
1. With the patient in standing position, one foot planted in front of the wall and the other staggered behind.
2. The front knee is in line with the second toe, and the great toe 10 cm away from the wall.
3. Balance is maintained by contact with the wall using two fingers from each hand.
4. Patient lunges forward, directing their knees toward the wall (in line with the second toe) until their knee touches the wall.
5. The foot is progressed away from the wall 1 cm at a time and the subject repeats the lunge until they were unable to touch the wall with their knee without lifting the heel from the ground.
6. Once the knee was not able to touch the wall, the foot is progressed in smaller increments toward the wall until the knee makes contact with the wall while the heel maintains contact with the ground.
7. Measurement from the great toe to the wall is to be obtained to the nearest millimeter.
More Than Just a Measurement
The measurement of ankle dorsiflexion is important for current status as well as to demonstrate progression with interventions. However, assessing the area or areas of restriction is another benefit to this screen. Since this is a weight-bearing assessment, it is more functional than a passive, open-kinetic chain measurement. To use this test to its fullest potential, use it to determine where your patient is experiencing symptoms or lack of mobility/flexibility.
If your patient describes “pinching” or discomfort in the anterior ankle, consider the talocrural joint. Assess and provide appropriate interventions to address any objective findings including the joint capsule, ligaments, or joints.
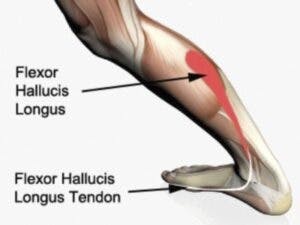
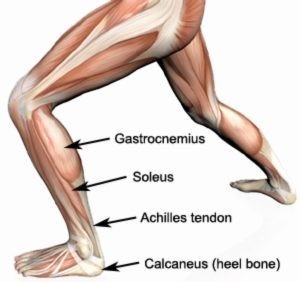
If your patient complains of tightness in the posterior lower leg, assess the soft tissues. Make sure you include the soleus and the flexor hallucis longus and flexor digitorum longus.
Test, treat, and retest to assure your approach is appropriate and effective. Follow up in clinic with corrective exercises to complement your manual techniques and provide the patient with a home excise program that will assist in maintaining/progressing any gains.